Forum, AMTA Methadone Conference, Phoenix, Arizona, October 31, 1995 )
European Methadone Association
27 rue de la Vanne
1050 Brussels, Belgium
Tel + Fax : 322 640 46 28
marc.reisinger@infoboard.be
SUMMARY
Methadone prescribing increased tenfold in the last four years in Belgium.
This has been made possible through involvment of general practitioners
in methadone treatment. Drug overdoses, crime and even presence of methadone
on the black market have decreased at the same time.
Introduction
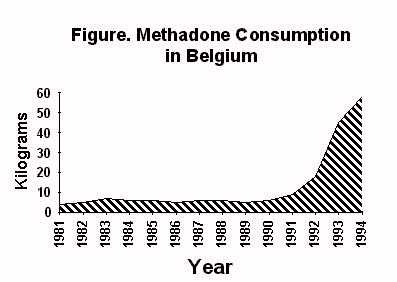
During the last four years, methadone consumption in Belgium increased
tenfold (From 6 kg/year in 1990 to 58 kg/year in 1994). This fact may seem
insignificant because it concerns a country with a population no higher
than that of New York City and whose precise geographic location may not
be known to everyone. However the Belgian experience might demonstrate
that it is possible to overcome certain limitations of methadone treatment
as it is generally practiced.
Legal confrontation
Methadone has been available with a prescription in pharmacies since the
1970’s. But physicians who began to prescribe it to addicts at the beginning
of the 1980’s, when the heroin epidemic was worsening, were often subjected
to disciplinary sanctions by the Belgian Medical Association and sentenced
by courts of justice.
At the beginning of the 1990’s a group of physicians, including myself,
requested that the Supreme Court revoke the Medical Association’s regulations
permitting the indictmemt of physicians prescribing methadone and other
substitution treatments. This request was granted. Subsequently, the regional
authorities of the French speaking part of Belgium began to encourage physicians
to treat opiate addicts with methadone. The authorities became aware of
drug addiction’s impact on criminality and on the AIDS epidemic. They knew
that it would be impossible to extend rapidly the number of methadone clinics
and they also wanted to avoid stigmatizing heroin addicts. To encourage
the treatment of addicts in normal settings, they allocated funds for training
sessions for general practicioners on treatment of drug addiction.
Consensus Conference
Another measure which permited a rapid expansion of methadone treatment
was the organisation of a Consensus Conference on Methadone Treatment by
our Minister of Health. The conclusions of the Consensus Conference were
sent to every doctor in the country, as new guidelines for methadone treatment.
They stated the following points :
- Methadone is an effective medication for the treatment of heroin addiction.
-
Methadone reduces heroin consumption and injection, reduces mortality
related to heroin addiction, reduces the risk of infection with HIV as
well as hepatitis B and C, improves therapeutic compliance of HIV-positive
drug addicts, facilitates detection of illness and health education strategies
and is associated with an improvement in socio- professional aptitude and
a reduction in delinquency. -
Prolonged treatment with proper doses of methadone is medically safe.
At present, methadone has not been shown to be toxic for any organ. -
There is no scientific reason to limit the overall number of heroin
addicts admitted for methadone treatment. -
Availability of methadone treatment should be increased to respond to
the need for such treatment, including by private practitioners. -
Psycho-social support is not compulsory and should be adapted to the
individual needs of patients.
These conclusions are in no way revolutionary on the scientific level,
but as official guidelines for methadone treatment, they represent a significant
innovation, compared to what happens in a lot of countries. Methadone is
now dealt with as an ordinary medication. Its effectiveness is recognized
without ambiguity. No longer is it considered an experimental treatment,
accessible only to a limited number of patients and subject to rigid controls.
No longer are patients required to have attempted previous withdrawal treatments.
Addiction can be ascertained by spontaneous withdrawal attempts recounted
during patients history. Urinalysis is done only following doctor’s decision.
It is specified in our new guidelines that dosage and duration of treatment
should not be limited, but adapted to each patient by the physician. It
is acknowledged that short-term methadone treatment are appropriate only
in certain very particular cases. Daily administration of methadone is
not compulsory, but recommended at the beginning of treatment and will
generally take place in a pharmacy chosen by the patient. The physician
is free to prescribe larger quantities of methadone at less frequent intervals,
depending on how the patient evolves.
Conclusion
The number of heroin addicts undergoing methadone treatment is increasing
and now reaches 5.000, out of an estimated total number of heroin users
of 20.000 to 30.000. More than 80% of these patients are being treated
by general practitioners. Hundred of general practitioners are currently
involved in methadone treatment. Most patients receive methadone provision
for one or two weeks, but the presence of methadone on the black market
has decreased, since less addicts are seeking methadone on the streets.
Drug overdoses and criminality have decreased. Thus the very flexible method
of prescribing methadone used today in Belgium seems to have resolved some
problems and does not seem to have created any.
Thank you.
Marc REISINGER
27 rue de la Vanne
1050 Bruxelles
Belgium
Tel + Fax : (322)640 46 28
